There are several causes of subnormal TSH including starvation, severe illness or cardiac events. In these cases, the best approach is to try to resolve the underlying problem. Another cause of subnormal TSH is a down-regulated hypothalamic pituitary thyroid axis. This can occur after a period of TSH suppression for example from taking high dose thyroid hormone or from periods of thyrotoxicity in early-stage Hashimoto’s thyroiditis (which the patient may not notice) or in Graves’ disease.
Long-term TSH suppression lowers the thyroid axis setpoint and fT3
This study demonstrates that long-term TSH suppression down-regulates the hypothalamic pituitary thyroid axis. i.e. for given fT3 and fT4 levels TSH is lower than expected. In this study the dose of L-T4 needed to achieve TSH suppression dropped from 2.96 μg/kg body weight to 2.25 μg/kg body weight over a period of 12.7 years. Some of this reduction was independent of aging. The fT3 / fT4 ratio also dropped significantly.

Results from my own trial
The following shows how a long-term suppressed TSH can down-regulate the axis and lead to reduced D2 activity causing hypothyroidism with ‘normal’ blood test results. It wasn’t intended as a prospective trial. After resolving my ARTH I tried to come off thyroid tablets, my thyroid has always been healthy and there seemed no reason why I should continue taking hormone.
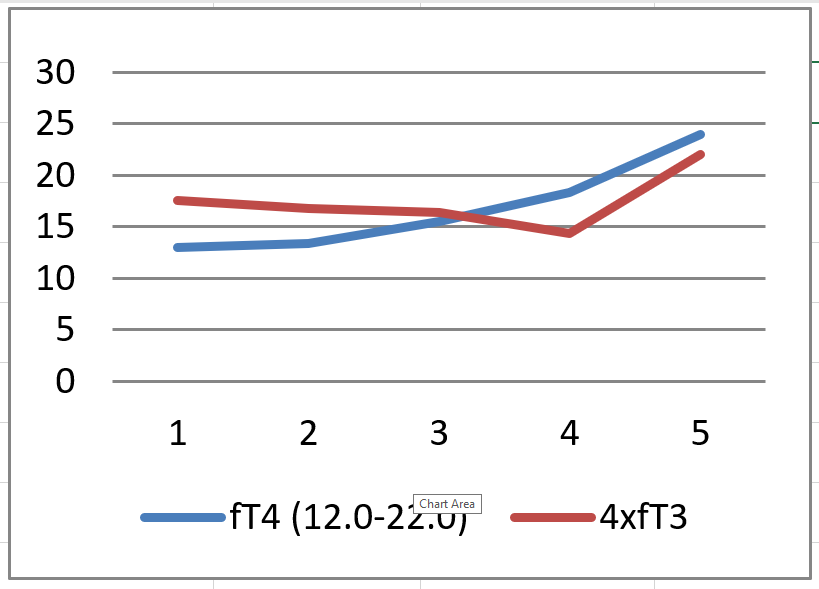
T3 in the blood is thought to be 4x to 5x as potent as T4, at least in terms of its ability to suppress TSH. (Note this does not apply to T3 and T4 in tablet form, they have different absorption rates and half-lives). As a very rough guide I set up: –
Set-Point Index = (4 x fT3) + fT4 with a Mean of 36.8 calculated from the mid-points of the reference intervals.
My % Mean from October 2000 (prior to any hormone treatment ) was 95%. At the time I had perfect blood test results TSH 1.0 (0.4 – 5.5) fT3 4.9 (3.5 – 6.5) fT4 13.3 (9.0 – 20.0)
The results below are from a period of about a year when I was on levothyroxine only. When taking no medication, I was hypothyroid with tiredness, mild IBS and experienced considerable back pain when walking. I was gradually getting worse – some consequences of hypothyroidism accumulate over time. Note that my Set-Point Index had fallen from 95% to 83%.
On 100 μg L-T4 I felt almost euthyroid but still had substantial cognitive impairment. The increase from 100μg to 125μg made no difference to my symptoms.

Patients 1 and 3 referred to earlier on in the Real Cases section have blood tests with the same reference intervals making it easy to calculate their Set-Point Indexes: –
- Patient 1 – Set-Point = 26.84, %Mean = 73
- Patient 3 – Set-Point = 26.89, %Mean = 73
By coincidence these two patients have similar results. Patients 2 and 4 have similar figures from different assays. These patients’ results are significantly worse than mine and so they will be much more hypothyroid. Bear in mind that not only is their combined serum hormone around 73% normal but the loss of T3 is largely due to reduced D2 activity. Their local T3 levels in D2 expressing tissues such as the brain and skeletal muscles will be very low. It’s hardly surprising they are in such a dreadful state.
We can plot my fT3, fT4 results graphically where the horizontal numbers 1, 2, 3, 4, 5 correspond to 0, 0, 50, 100, 125 mcg L-T4: –
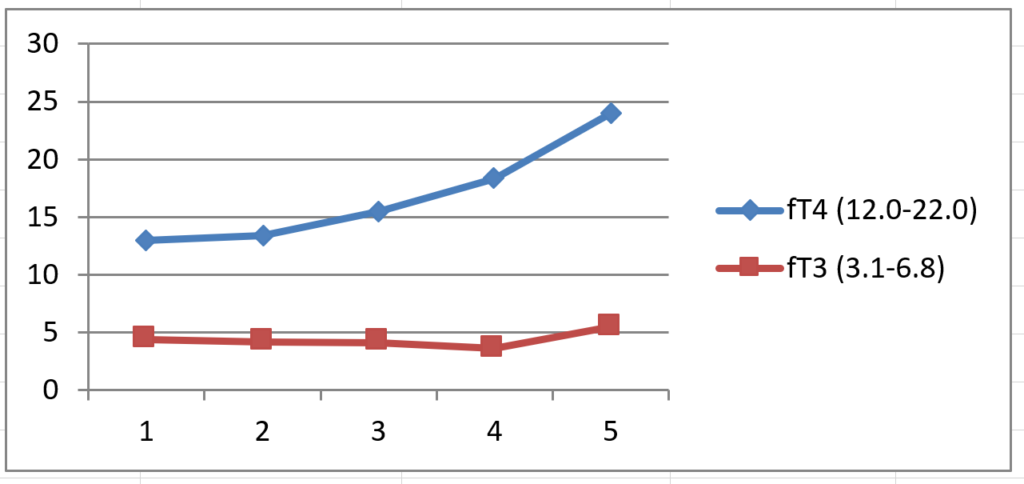
We can see that as fT4 rises fT3 falls. In healthy people fT3 tends to remain fairly constant or increase. I suspect the increase in fT3 on 125 mcg L-T4 was due to D1 activity taking over when the hormone levels are high, there would have been very little D2 activity at this stage because TSH was very low and fT4 high. There was no clinical benefit in the change from 100 mcg to 125 mcg L-T4, the extra 25 mcg did not help at all.
Since subjects with a normal thyroid axis will have more D2 activity there will be a greater degree of overlapping D1, D2 activity giving more stable serum and intracellular T3 levels. (An interesting conjecture is that this disjoint between D1 and D2 in patients with a subnormal TSH may make them a useful cohort for studying deiodinase).
Subnormal TSH does not respond to levothyroxine only therapy
If T4 medication is given to patients with a subnormal TSH some or all of the benefit will be lost as a consequence of a low TSH being reduced further, leading to even lower D2 activity and lower intracellular T3. In some cases, the T3 reduction will have greater effect than the increased T4. ironically if these patients are prescribed levothyroxine, they become more hypothyroid.
My experience is that L-T4 does not help, it gives minimal improvement. Some tissues prefer to take in T4 using D2 to convert it to T3 (e.g. the brain). If D2 is not functioning correctly supra-physiological levels of T3 will be needed to get adequate T3 to these tissues. I have to take 40 mcg L-T3 daily to achieve near normal brain function and avoid muscular pains. I take 25 mcg L-T4 daily because it helps avoid a slow gut and also because T4 may have functions we are not aware of. It makes sense to retain a little T4 just in case. Clearly there is the potential for tissues that do not express D2 to become thyrotoxic. This is a concern, but I have not noticed untoward effects. Ideally, we would restore a normal axis and discontinue hormone treatment (if the thyroid is OK).
We’ve covered a lot of ground so here’s a Summary.