The nature of collagenous colitis (CC) is similar to mechanical and electronic systems that can be switch ‘on’ and ‘off’ by small inputs. For example, the Torbeck valve which replaces the much larger ballcock.
Once collagenous colitis is switched ‘on’ it tends to stay ‘on’. Budesonide therapy and faecal stream diversion switch ‘off’ CC but the ‘on’ state resumes after these therapies are stopped. We must find out why this happens, find the mechanism which sets the switch.
This simplistic approach enables us to isolate the problem. We tend to be overawed by medical problems and miss simple solutions.
Features of Collagenous Colitis
- Increased collagen layer thickness.
- Budesonide is an effective treatment restoring normal collagen layer thickness.
- The collagen layer recovers after diversion of the faecal stream suggesting the presence of a noxious factor.
- Collagenous colitis is associated with bile acid malabsorption (BAM) and budesonide reduces BAM. Bile acid may be the noxious factor.
Proposed Mechanism of CC
An insult to the gut triggers CC leading to BAM. BAM causes inflammation which sustains CC.
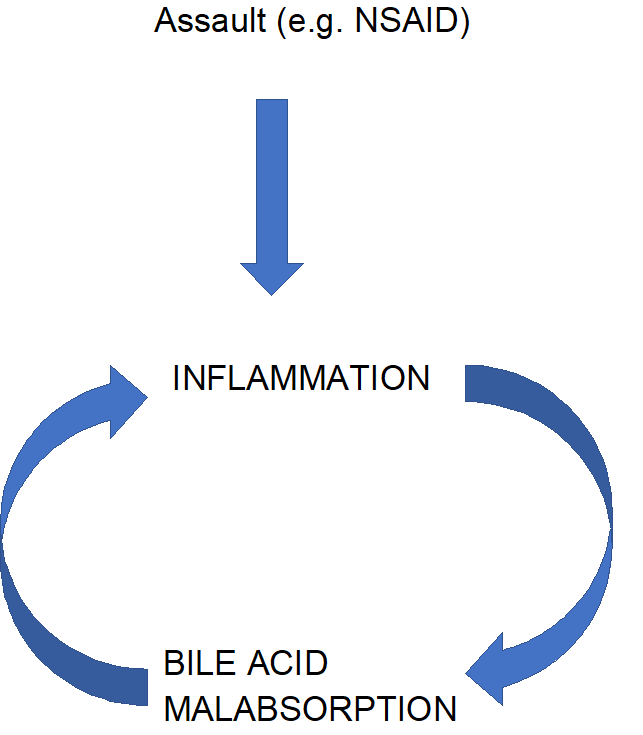
There is an assault on the gut which causes inflammation and bile acid malabsorption. Bile acids further inflame the gut leading to a pathogenic vicious circle. To cure CC we must break the circle.
Budesonide is a corticosteroid hormone with local action. Hormone treatment may suppress endogenous hormonal action by e.g. down-regulating receptors or supressing secretion. These effects can take time to wear off. Thus, when budesonide treatment is discontinued the gut is vulnerable, exposed to bile acid and CC relapses. If we protect the gut from bile acid whilst budesonide therapy is tapered down, we may be able to cure CC.
Protecting the gut from bile acids during budesonide withdrawal.